

Contra TFP on Factitious Disorder
Contra TFP on Factitious Disorder
and a short part deux on signal detection

This is primarily a response to ‘Take Care of Münchausen syndrome’ and if you came for the punchline, here it is: the difference between malingering and factitious disorder is indeed in the motivation, but that difference isn’t ‘conscious vs unconscious’, it’s ‘tangible vs intangible’.
If it weren’t for the adverse Substack norm of paywalling comments sections I’d have been able to address this in a less megaphonic style, but what can you do? Some things are too much for this reply-gal to abide. TFP’s post1 starts to go off the rails in paragraph number 2:
There is a psychiatric illness called factitious disorder. Factitious disorder, previously referred to as Munchhausen [sic] syndrome, refers to the unconscious motivations that lead someone to attempt to feign illness consciously. This acknowledgment of the word “consciously” is followed by “for unconscious reasons.” This is the only time the unconscious appears in the fifth edition diagnostic and statistical manual. People’s unconscious motivations for conscious actions are only mentioned here in DSM-5. These are not people who are simply faking. People who know they’re faking—imposters— we have a different name for that. That’s called malingering.
At best this is written in a way that is misleading, and at worst—the last two sentences in isolation—is plainly incorrect. I’m going to consult a few sources here, but let’s start with the one linked above. There are two claims I’m taking issue with. One is that the motivation for factitious disorder2 is necessarily unconscious. The other is that people with factitious do not know that they are faking. Here is the first paragraph of the linked resource, emphases mine:
Factitious disorder is a serious mental disorder in which someone deceives others by appearing sick, by purposely getting sick or by self-injury. Factitious disorder also can happen when family members or caregivers falsely present others, such as children, as being ill, injured or impaired.
Factitious disorder symptoms can range from mild (slight exaggeration of symptoms) to severe (previously called Munchausen syndrome). The person may make up symptoms or even tamper with medical tests to convince others that treatment, such as high-risk surgery, is needed.
Factitious disorder is not the same as inventing medical problems for practical benefit, such as getting out of work or winning a lawsuit. Although people with factitious disorder know they are causing their symptoms or illnesses, they may not understand the reasons for their behaviors or recognize themselves as having a problem.
People with factitious disorder know they are faking (contra claim 2), and they may or may not know why (contra claim 1). They lie and intentionally deceive others, and they know that that is what they are doing. They are not somehow confused about whether their lies constitute lies. The difference between factitious disorder and malingering is not insight into one’s motivations, it is the nature of those motivations. In cases of malingering, the benefit is objective and the appeal is obvious—money, time off work, child custody, illicit drugs, etc. Owing to the tangible and secondary nature of these rewards, people who are malingering tend to be aware of their own motivations. That conscious awareness is required to orient them in the direction of the desired reward. In cases of factitious disorder, the benefit is psychological and inherent to being seen as sick—often thought to be the assumption of the ‘sick role’. It’s certainly the kind of pattern a person can fall into without intent, rather than calculating their way toward. Still, the sufferer of factitious disorder is aware of what they are doing and that others would understand it as deception if they were aware. They may or may not have insight into why they are doing it. There are important etiological and prognosticative differences between malingering and factitious disorder. For one, malingering outside of psychopathy3 is usually isolated and situational, while factitious disorder tends to be refractory. But that difference does not inhere in insight, it inheres in whether the motivation is practical and contingent to one’s circumstances, or (presumptively) some kind of soul-sucking wound the sufferer is trying to salve. Let’s turn to StatPearls on Münchausen syndrome:
When differentiating Munchausen from other psychiatric disorders, it must be remembered that Munchausen patients have insight into their disorder and are aware that they are fabricating their illness.
Having established this, let’s take a look at paragraph three (emphasis not mine):
Malingering is the medical term for lying because you want to get something out of it. Usually, when people are malingering, which is lying, they are defined to know that they are lying and why they’re lying. Factitious disorder does not invoke the knowledge of one’s motivations. Explicitly, factitious disorder exists because of the human ability to avoid seeing one’s motivations—even while seeing one's behavior.
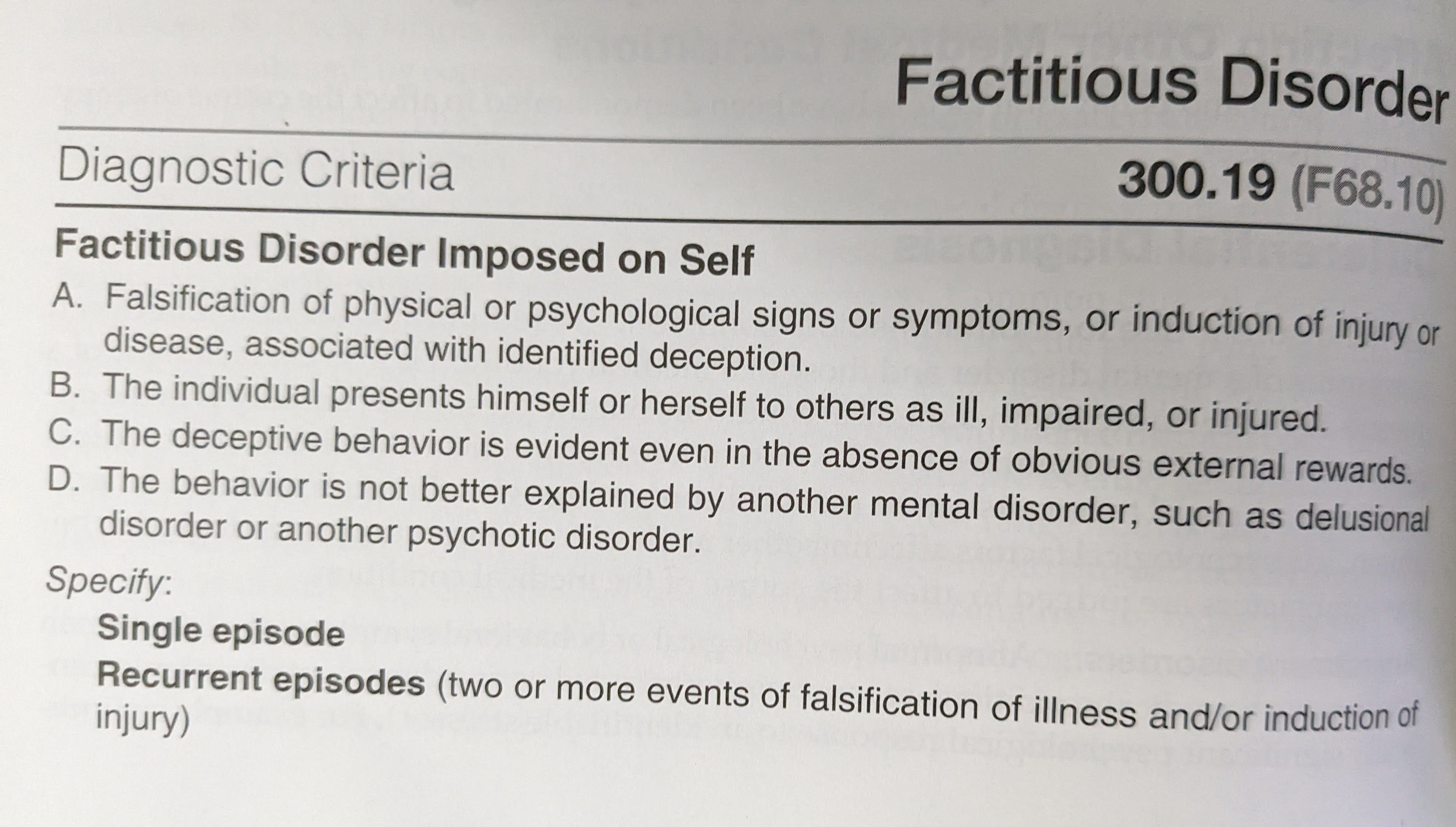
I’m uncertain where this explication is coming from! It certainly isn’t the DSM-5 criteria for factitious disorder (nor any of the text, as we shall see):
“1) Intentional induction or falsification of physical or psychological signs or symptoms
2) The individual presents themselves as ill, impaired or injured to others
3) The deceptive behavior persists even in the absence of external incentives or rewards
4) Another mental disorder does not better explain the behavior”
Maybe we’re closer to being correct about the definition of malingering? Alas. Let’s try StatPearls again (emphasis mine):
Malingering is falsification or profound exaggeration of illness (physical or mental) to gain external benefits such as avoiding work or responsibility, seeking drugs, avoiding trial (law), seeking attention, avoiding military services, leave from school, paid leave from a job, among others. It is not a psychiatric illness according to DSM-5 (Diagnostic and Statistical Manual of Mental Diseases, Fifth edition).
Here’s the APA Dictionary of Psychology on malingering :
the deliberate feigning of an illness or disability to achieve a particular desired outcome. For example, it may take the form of faking mental illness as a defense in a trial, faking physical illness to win compensation, or faking an injury or misinforming people of one’s state of rehabilitation to avoid practicing or playing sport. Malingering is distinguished from factitious disorder in that it involves a specific external factor as the motivating force.
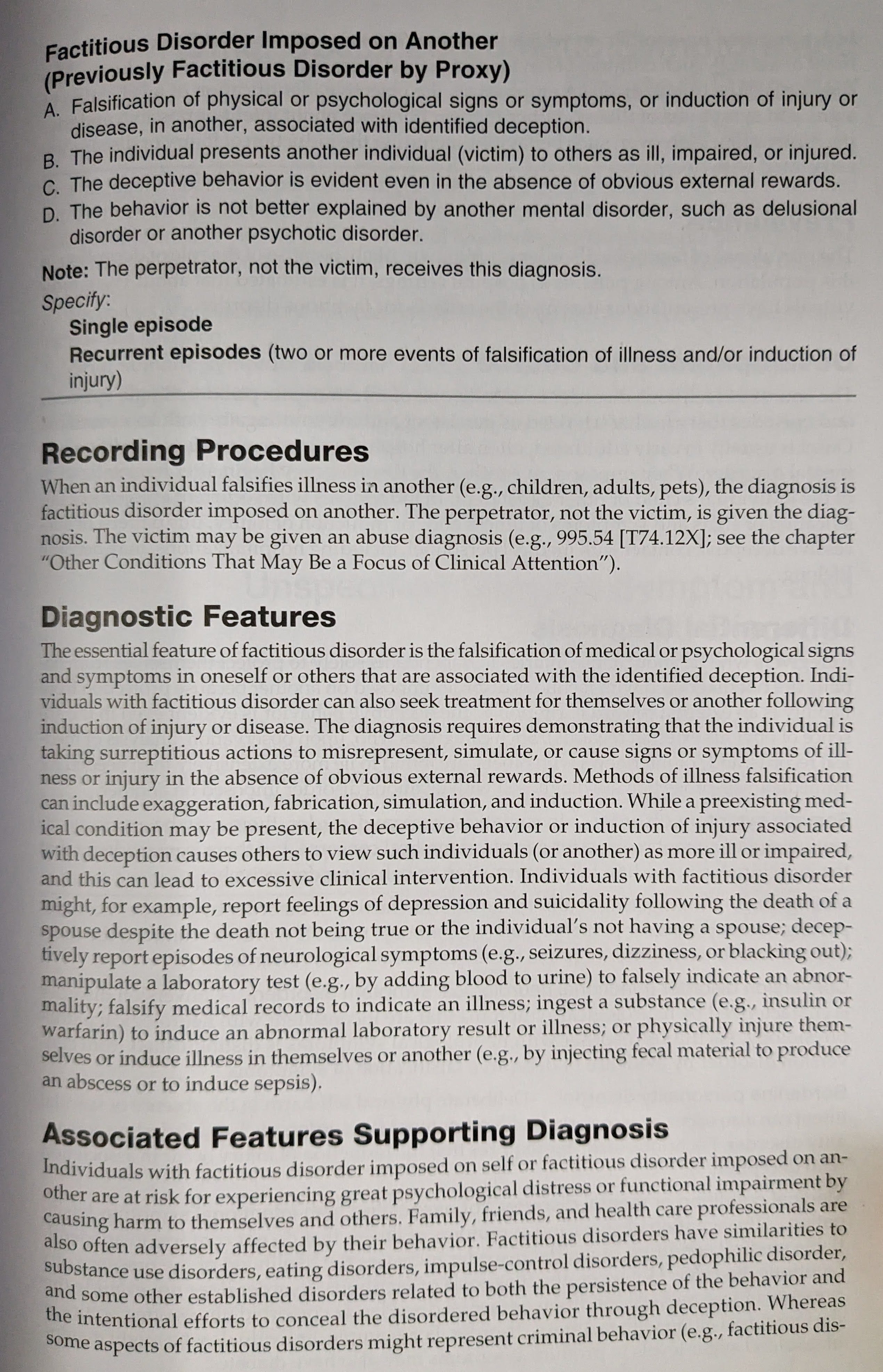
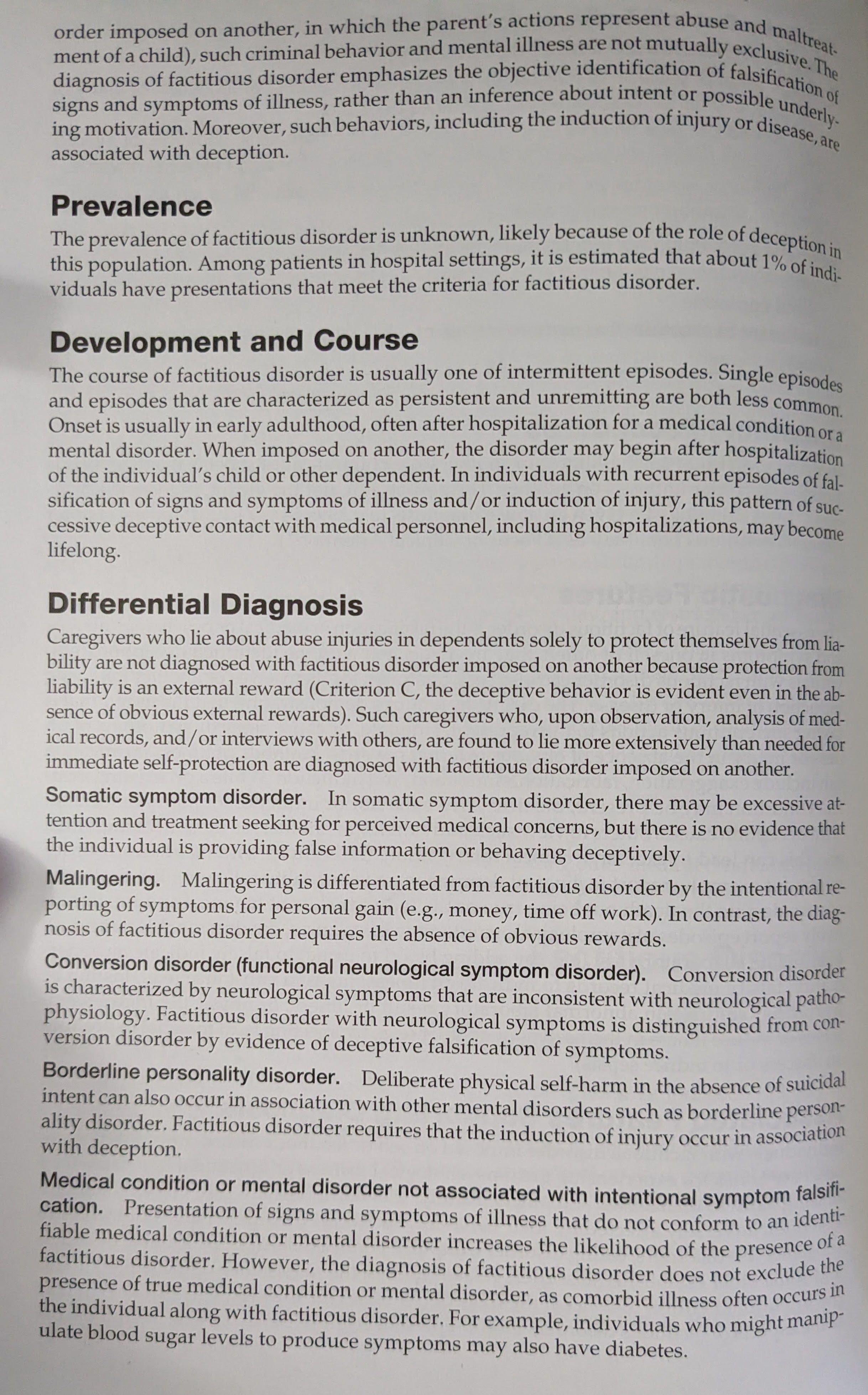
I could do this all day, because this is not an issue of debate or finesse. The criteria used to distinguish factitious disorder from malingering are straightforward and they are not what has been claimed. And when the most cursory inquiry illustrates this it’s difficult to know what could have gone wrong here. I was so curious that at this point in writing I went rutting around in the garage for my own copy of the DSM-5 (languishing with all my other books at present) to find the relevant subsection and the reference to unconscious motivations. But I cannot find this ostensible single instance of the word ‘unconscious’ anywhere under the heading of factitious disorder, so I have not been enlightened on this point. It is possible I’ve overlooked it, so I’ve reproduced the entry as it appears in my physical book. It’s also possible it appears in the DSM-5-TR, although I can’t find any references to such changes.
I happen to have read some of Mark Feldman’s work on factitious disorder. Like a lot of people who are interested in psychology I became intrigued enough by the intentional fakery of medical conditions to do a deep dive. A few of the patients whose stories he relates have surprising insight into their own motivations—that is to say that, in addition to knowing exactly what they are doing, they know what about it appeals to them and why they persist, they are able to predict that they will continue the behavior. Some will even say they wish to but cannot stop.4
This is not at all an instance of anosognosia—the inability to know that one is sick—even under the most generous psychology-pilfered definition. (If I had my druthers psychiatry would politely hand the term ‘anosognosia’ back to the neurologists with some apologies for the damages—this fascinating phenomenon is simply not part and parcel with what happens when schizophrenics deny their illness5 or people with depression assert and believe that they are fine—but that’s for another day.) It’s not even an instance of the inability to really know why one does what one does, which (as the piece does lope around to) is also known as the human condition. This part of the post I largely agree with:
Our brains are extremely good at telling us stories about what is real. We are wired to believe those things. Doubting your reality? That’s called paranoia and can be a symptom of illness. We’re usually good in a state of relative wellness at believing the stories our brains tell us. Just like computer programmers worry about artificial intelligence and how confident it can be when presenting its findings, our brains— original intelligence—have similar programming. Conviction about the real is a feature, not a bug, for humans.
Sometimes, our conviction about the real has a glitch. These glitches are hard to understand because we’re all running the “conviction about what’s real algorithm” in our heads.
Misunderstanding ourselves is our human inheritance. It just has very little to do in particular with factitious disorder, and factitious disorder has very little in particular to do with it. When you are having a really bad reality glitch we call it a delusion. It’s possible to have them about your health, as in delusional parasitosis. Factitious disorder patients are not as a rule delusional—and this is one rare instance where it would be easier to understand the phenomenon if the patient were simply delusional.
It’s a sick thing. It is a sick thing to do to someone somebody else. In this context, I argue that the word sick isn’t intended as an insult. The real sickness is a lack of insight on the part of the person doing the sick-making of their child.
No, actually. The real sickness is the psychological rent compelling the abusive behavior, whether or not the patient is aware of its nature. And when people with factitious disorder lack understanding of why they do what they do, this is no more the source of their pathology than the ordinary lack of understanding of our own motivations that we all display. (This is what becomes of stealing terminology from the neurologists! The road to hell is paved with Greek and Latin.)
One of the reasons that I think it is important to stress that people with factitious disorder are aware that they are engaging in deception is the existence of the entire class of somatoform disorders. In a somatoform disorder, there is no deception at all. The problems aren’t faked, and the person isn’t lying. They are cases of genuinely experienced symptoms whose cause is psychological6 rather than physical. Functional neurological disorders can be especially dramatic—think seizures and paralysis—and are neither faked nor caused by the kinds problems in the nervous system that typically cause seizures and paralysis. By providing that people with factitious disorder do not know that they are lying, are not accurately described as fakers or imposters, it becomes difficult to distinguish between someone with FND who thinks they are having a seizure and someone who falls to floor and causes themself to flop about. Again, the only difference between factitious disorder and malingering in the latter case is whether you’re flopping about to get out of jury duty or just because you like it when the nurses help you up off the ground.
It’s unclear what these misrepresentations are in service of. I don’t think that you need to lack insight into your condition to be deserving of compassion and care, but I hazard that an attempt to include people who abuse their children in this way in the sphere of empathy (and, to be clear, you should include them in the sphere of empathy) might be what’s motivating an insistence that they don’t even know that abuse is occurring:
Fundamentally, I’m a scientist. I’m skeptical. But I’m human, and so I believe—we all do! This story of Factious [sic] Disorders? It is about that “reality check” system that lets us believe. People can be unable to see the truth, even when it’s right in front of their face. Not because they’re bad or wrong. Because we are human.
I agree that sufferers of factitious disorder are not ‘bad and wrong’. Another part of the human inheritance is willingness to hurt others, even those we love, for our own gain. When the perceived gain is large enough (as in addiction) this doesn’t call out for any special explanation. Our difficulty in understanding and relating to FDoiA lies in how we appraise the relevant gain. TFP’s characterizations, that FD patients necessarily lack insight into what they are doing and are incapable of knowing their own motivations, are flatly wrong, a point which I’ve now belabored.
I entreat TFP to correct their post for the benefit of their many readers.
Update: Not long after writing this I listened to a podcast—Nobody Should Believe Me—which provided factual information that was left out of the Netflix documentary, substantially revising my opinion on the case. I no longer recommend watching the documentary if it’s the only thing you feel you’ll have time for. I’m leaving this section unedited, but I aim to follow up with another post on this constellation of topics.
I watched ‘Take Care of Maya’ myself this weekend, on the heels of the $261 million judgment Maya Kowalski’s7 family was awarded following her mother’s suicide. As someone who’s read a lot about factitious disorder(/imposed on another) over the years and who takes the condition seriously, I expected to be as offended as I knew some other ‘FD enthusiasts’ to be. I had no such reaction; I didn’t find that the documentary trivialized or even cast doubt on the validity of the diagnostic category. It seemed to be about something very different—bureaucratic overreach and the helplessness of people who become targets of the state however whimsically, a broad phenomenon that shares themes with criticisms of criminal justice as currently practiced in the US. Some insist that Maya Kowalski was in fact a victim of FDoiA, and while this is technically possible, it’s also the conclusion you’d draw if falling into the failure mode I think of as ‘Either-Type-Error-Blindness. Also known as failing to treat a signal-detection problem as such. People who attend to one class of error (either false positives or false negatives) can be reluctant to admit the existence of the other class. Sometimes both classes are large! It is possible to be bad at classification in both directions!
Consider a generic case of a parent taking their child to the doctor. In the vast majority of cases, the doctor and the parent come to an agreement: either something is wrong with their child, in which case investigations and treatments ensue, or something is not, in which case everyone is relieved. When the assessment of the doctor and parent diverge, it’s actually the assessment of the doctor and the nature of reality that constitutes the relevant 2x2. In the case of TCoM, the Kowalski’s assert that identifying Maya as a victim of FDoiA was a Type-I (false positive) error. The doctors asserted that it was a ‘hit’—a correct detection. Some detractors assert that the doctors must be correct on the grounds that they make many Type II errors (false negatives), routinely failing to identify the estimated 1% of hospital admissions that involve some kind of FD. Or, less strongly, that it’s inappropriate to highlight an instance of a Type I error when the industry is still churning out Type IIs and hardly anyone is aware. I assert simply that you can both miss a lot of targets and shoot a lot of things you didn’t mean to shoot—often the two are correlated owing to the underlying causal factor of ‘being bad at shooting’. The situation is not always well-modeled as moving the signal detection threshold along a static distribution, where every additional correct rejection comes at the expense of additional Type II error, and so on. This is especially so if you adopt hasty and ill-suited decision criteria in an effort to overcorrect for past mistakes, as I think may have been in play in this case. Maya’s mother Beata was by all accounts a forceful personality who was willing to contradict her daughter’s doctors when she felt she knew better. I’ll leave you with this excerpt from The Cut’s piece on the subject, which has stayed with me, and gives you a sense of how the doctors at the hospital thought of Maya’s mom, and what kinds of considerations they might have been bringing to bear in their diagnoses:
Laura Vose, a doctor at the hospital, texted her colleague Beatriz Teppa Sanchez. “Ketamine girl’s mom committed suicide yesterday. Sorry to say my prediction was correct.” She appears to have meant that Beata was mentally ill.
“Omg,” Teppa Sanchez wrote back. “This is terrible … I know we did the right thing. But this is really fucked up. I feel bad.”
“Don’t know all the details but I think the courts and psychiatrists finally called it what it was,” Vose typed. “I had another mother do this same thing.”
I don’t pretend it’s an objective account, and I would have liked to know much more about what the clinicians at the hospital were thinking, but the documentary is well worth a watch.
I obviously know the name of the author but in an effort to avoid seeming like I’m courting confrontation I’ll refer only to the name of the blog here, and only as an acronym.
I will be using ‘factitious disorder’ rather than Münchausen syndrome throughout, but there’s no elision—the former replaces the latter, though you still see it around. FD and FDoiA will refer to factitious disorder and factitious disorder imposed on another, respectively.
Shorthand, replace with whichever denomination of immorality syndrome you prefer if need be.
This is all admittedly on recollection, as I don’t have access to those texts anymore. But since the nature of insight and remorse in FD was one of things I was most interested in sussing out, I don’t think I am wholly misremembering.
One thing that’s under-appreciated about psychosis is the ability to have a kind of dual-track awareness of what’s happening to you. On one ledger you keep track of the delusional content and its implications, and on another you’re simulating ‘what other people are thinking about me’ and the implications of that. You can simultaneously know that you are doing a psychosis, think it to be psychosis, and also believe in the delusions that make such distinctions at best irrelevant, at worst inverted in desirability.
Some accounts are agnostic about cause and stipulate only that the presented syndrome is incompatible with physiologic injury.
Unfortunately her surname is variously misspelled as Kowlski and Kowolski throughout TFP’s post.